Burn Injuries Lawyer
A severe burn.
Nothing can prepare you for it. No words or pictures can fully describe it. It is, simply, one of the worst experiences imaginable.

Hi, my name is Fred Pritzker. I am a lawyer who helps burn victims and their families. I have helped some amazingly brave people get the money needed to move on with their lives. One of my clients lost both an arm and a leg. His settlement money will help him have the best prosthetics (artificial limbs) and medical care available. He said it best: “I’m still alive, and I get to spend the rest of my life with my family. And we’re going to be happy the rest of our lives.”
Many lawyers advertise for burn injury cases, but not all of them have won large settlements. I help people throughout the United States and have won settlements over $10 million. You can contact me to find out how much your case is worth and what steps we can take together to get you full and fair compensation.
Contact Attorney Fred Pritzker Using the Form Below
Third and Fourth-Degree Burns
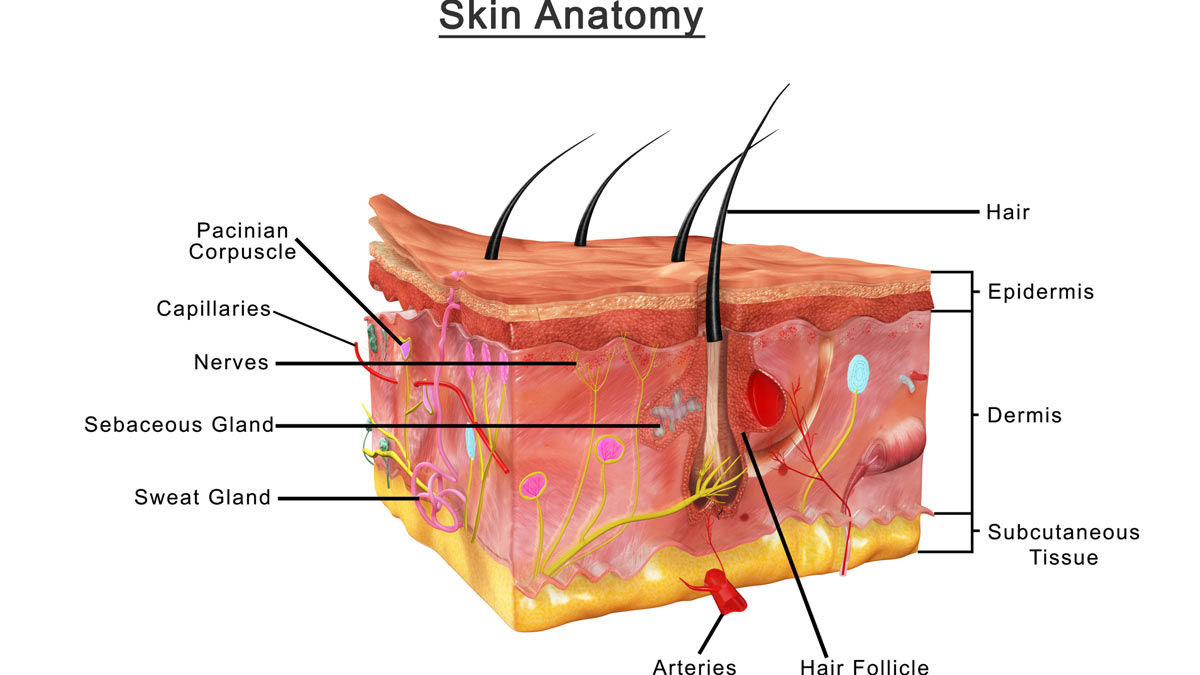
As we learned in school, human skin is the largest of the body’s organs. It prevents pathogenic microorganisms from entering the body, retains fluids within the body, regulates body temperature, affects the composition of body fluids, contains nerves that allow us to sense and interact with the world around us, and synthesizes Vitamin D.
A third-degree burn, also known as a full-thickness burn, destroys the entire thickness of the skin. Thus, all the functions of the skin over the badly burned area are lost as well. Nerves, blood vessels, sweat glands, sebaceous glands, and hair follicles are decimated.
If the burn damage is even deeper than the entire thickness of the skin – into the subcutaneous tissue, muscle or bone – it’s classified as a fourth degree burn.
Smoke Inhalation and Burn Shock
Initial evaluation of severely burned individuals involves assessment of breathing. Smoke inhalation or thermal injury to the airway requires immediate intervention. Without it, brain damage and death quickly ensue.
The effect of a severe burn is not limited to the area of skin damage or skin loss. With burns that affect 20% or more of the total body surface area (TBSA), “burn shock” results. Burn shock is the product of a massive inflammatory response that causes leakage of fluids and salts from blood vessels into the non-functional areas between cells (known as the “third space”). If too much fluid is lost, the heart is unable to maintain life-sustaining blood pressure, organs shut down, and the patient dies.
To counteract burn shock, IV fluids must be administered. These fluids, along with “third spacing,” produce edema (swelling). However, because the surrounding burned tissue is no longer as elastic as normal skin, it acts as a “plaster cast” compressing and constricting blood flow and cardiac output as well as nerve and organ function. Without surgical intervention, affected sites will suffer irreversible damage and the patient may die.
The surgical procedure necessary to prevent this cascade is called an escharotomy. It involves cutting into the skin and underlying tissue causing it to spread open. This releases the pressure and constriction which allows bodily function to normalize. It’s also for that reason that surgical wounds from escharotomy are not closed with sutures or staples. The wounds have to remain open, but that also increases the risk of infection that’s ever present with severe burns.
Burn Treatment
Initial treatment of severe burns includes wound cleaning, removal of burned tissue, and application of topical antibiotics and sterile bandages. Dressings must be changed on a frequent basis, as often as every eight hours. Even with medication, the process is extremely painful and the fact that it must be repeated on an ongoing basis over a long period of time makes it even worse.
During this time, maintaining appropriate fluid levels and supporting the increased nutritional needs of the patient is critical. That’s because the body’s rate of metabolism increases along with the ongoing inflammatory process and wasting of lean body mass. This process further impairs wound healing and makes the patient more susceptible to infection.
The gold standard for treatment of severe burns involves early (often within 24 – 48 hours post-injury) surgical intervention consisting of cutting away burned tissue and covering the wound with replacement skin or a skin substitute.
The patient’s own skin taken from an unburned donor site (autograft) is usually preferred, but if the burn area is extensive there may not be enough harvestable skin to achieve skin closure. In such cases, temporary coverage may be accomplished with tissue from another person or a cadaver (allografts) or with tissue from an animal (xenograft).
Artificial skin substitutes are also used for coverage. This involves placement of a thin, film-like material that protects the wound from infection and helps with temperature regulation and fluid retention. The material also acts as a scaffold to facilitate skin growth. When the process is completed, part of the film is surgically removed and replaced with grafted skin from donor sites on the patient’s body.
A surgical instrument called a dermatome is used to slice thin layers of undamaged skin from donor sites that are meshed (allowing the skin to stretch and cover a larger area) and then surgically placed over burn sites. In time, and barring infection and complications, the donor skin permanently covers the burn area.
Despite state-of-the-art care, if burns affecting the toes, feet, legs, fingers, hands, arms, ears, nose, or any other part of the body not absolutely essential for life, are too severe, amputation is required.
All of this cleaning, scrubbing, cutting, harvesting, and dressing wound sites which may occur over days, weeks or months is painful, often excruciatingly so. Pain medication is obligatory but also problematic. Hallucinations, respiratory distress, and long-term addiction issues may occur.
Burn treatment also includes physical therapy necessary to regain function and prevent further skin contraction. Special compression garments may also be required for treatment of hypertrophic (raised) burn scars which affect a burn survivor’s level of function.
Psychosocial Aspects of Severe Burn Injuries
The psychosocial aspects of severe burn injuries are significant and exist (and change) throughout the three stages of recovery (resuscitative/critical stage, acute stage, and during long-term rehabilitation).
Critical Stage
During the critical stage, the patient is struggling to survive. S/he exists in an intensive care environment with no privacy, little physical function, often in great pain, on high doses of drugs, and all the while lying in a hospital bed for a prolonged period of time. Sleep is problematic. The profound monotony and under-stimulation is interspersed with the hyper-stimulation of pain and scary medical procedures and operations. Interaction with family members who are stressed and anxious often intensify the patient’s own negative feelings.
Acute Stage
During the second stage (acute), the patient is more aware of the physical and psychological aspects of his/her injuries. With greater awareness (and often greater physical pain due to a decrease in sedation), anxiety and depression symptoms start to appear. The intensity of depression and anxiety symptoms is often correlated with the severity of the burns. Sleep deprivation and pain control issues remain. Feelings of loss and the beginning of the grieving process commence as the impact of the burns starts to sink in.
Rehabilitation Stage
Following release from the hospital, the long term rehabilitation stage begins. Outpatient physical therapies, use of compression garments, undergoing additional medical procedures, re-integrating into family and work life, confronting the issues of everyday life, and dealing with the physical and emotional realities of burn injuries (ongoing pain, itching, temperature regulation issues, dreams and flashbacks, etc.) have a significant and often disorienting impact on the lives of severe burn survivors (and their families) during the remainder of the first year of recovery and beyond.
People with severe burns, especially if they involve the head, face and hands, experience difficulty coping with the change in their appearance. Chronic anxiety, depression, withdrawal from activities, unwillingness to be seen in public, nightmares, flashbacks, problems with sleeping, and the feeling that affected body parts “don’t belong” are signs and symptoms associated with burn-related disfigurement and may also constitute Post-Traumatic Stress Disorder (PTSD)
Getting Just Compensation
At Pritzker Hageman, we understand the intense physical and emotional suffering experienced by our burn-survivor clients. We also understand the incredible investment of time and effort necessary to recover and allow burn survivors to move on with their lives.
That’s why, in addition to obtaining just compensation and holding wrongdoers accountable, our job is to provide hope and understanding for our clients. We’ve helped so many burn survivors reclaim their lives, accept the challenges, and embrace the future.

Leave a Reply
Want to join the discussion?Feel free to contribute!